Peripheral vascular disease commonly affects the arteries supplying the leg and is mostly caused by atherosclerosis. Restriction of blood flow, due to arterial stenosis or occlusion, often leads patients to complain of muscle pain on walking (intermittent claudication). Any further reduction in blood flow causes ischaemic pain at rest, which affects the foot. Ulceration and gangrene may then supervene and can result in loss of the limb if not treated. The Fontaine score is useful when classifying the severity of ischaemia. Although many patients with claudication remain stable, about 150 200 per million of the population progress to critical limb ischaemia (Fontaine III or IV) each year. Many patients with critical limb ischaemia can undergo revascularisation, which has a reasonable chance of saving the limb. A recent audit by the Vascular Surgical Society found a success rate of over 70% for these patients. However, many patients still require major amputation. Rehabilitation of elderly patients after amputation can prove difficult, with high community costs. Critical limb ischaemia has been estimated to cost over £200m a year in the United Kingdom.
Intermittent claudication
History and examination
A history of muscular, cramp like pain on walking that is rapidly relieved by resting, together with absent pulses, strongly supports the diagnosis of intermittent claudication. Disease of the superficial femoral artery in the thigh results in absent popliteal and foot pulses and often causes calf claudication. Disease of the aorta or iliac artery results in a weak or absent femoral pulse, often associated with a femoral bruit. Disease at this level may cause calf, thigh, or buttock claudication.
The dorsalis pedis artery lies superficially on the dorsum of the foot, although its position varies considerably. The posterior tibial artery lies deeper behind the medial malleolus. Many healthy people have only one foot pulse. The popliteal pulse can be difficult to palpate in muscular patients. A prominent popliteal pulse suggests the possibility of a popliteal aneurysm.
Differential diagnosis
The pain of nerve root compression can be mistaken for vascular claudication. A careful history can usually distinguish nerve root compression, especially sciatica due to compression of the lumbosacral root. However, compression of the cauda equina due to spinal stenosis can be more difficult to diagnose. This condition usually causes pain that radiates down both legs. Although the pain is made worse by walking, it also comes on after prolonged standing and is not rapidly relieved by rest, unlike vascular claudication.
Investigation
There are many causes of leg pain that can occur in the presence of asymptomatic peripheral vascular disease.
Therefore, the absence of pulses does not necessarily imply a causal link. Furthermore, the presence of pulses at rest does not exclude symptomatic peripheral vascular disease. A good history together with an ankle brachial systolic pressure index of less than 0.9 confirms the diagnosis. Exercise testing provides an objective measurement of walking distance, and highlights other exercise limiting conditions such as arthritis and breathlessness. However, exercise testing takes time, and many patients find it difficult or impossible to walk on a treadmill. Only those with a good history of claudication and normal resting ankle brachial
systolic pressure indexes require an exercise test. Duplex ultrasound scanning is useful for delineating the anatomical site of disease in the lower limb. Many hospitals still use arteriography for this purpose or when the results of duplex scanning are equivocal. This invasive and expensive investigation should not be requested unless there is a plan to proceed with revascularisation, if possible.
Principles of treatment
Intermittent claudication seems a relatively benign condition, although severe claudication may preclude patients from manual work. The risk of generalised vascular disease is probably more important. Patients with claudication have a three times higher risk of death compared with age matched controls.Modification of risk factors is therefore vital to reduce death from myocardial infarction and stroke. All patients should be advised to stop smoking and take regular exercise. They should also be screened for hyperlipidaemia and diabetes. Patients with peripheral vascular disease benefit from regular chiropody, and those with diabetes should attend a foot clinic.Obesity reduces exercise capacity, and losing weight will improve the walking distance.
Exercise programmes
A recent meta analysis of 21 supervised exercise programmes showed that training for at least six months, by walking to near maximum pain tolerance, significantly improved pain free and maximum walking distances. The only controlled trial comparing an exercise programme with percutaneous transluminal angioplasty found that exercise was better. Exercise programmes are cheaper than percutaneous transluminal angioplasty or surgery, although long term compliance seems poor.
Endovascular techniques
The number of percutaneous transluminal angioplasties performed for claudication has risen steeply in recent years. In some situations endovascular techniques have virtually replaced conventional surgery. Percutaneous transluminal angioplasty seems best suited for stenoses or short occlusions of the iliac and superficial femoral vessels, with one year patency rates of 90% and 80% respectively. Angioplasty carries a small but definite risk of losing the limb because of thrombosis or embolisation, and patients should be informed of this risk.
Metallic stents push back the atheroma and improve on the initial lumen gain after angioplasty alone. The indications for iliac stents include a residual stenosis or dissection after angioplasty and long occlusions, but there seems little evidence to justify their routine use. Deployment of stents more distally has produced disappointing results due to high restenosis rates.
Surgery
The role of bypass for longer arterial occlusions remains poorly defined because of a lack of proper trials comparing it with percutaneous transluminal angioplasty and conservative treatment. Polyester (Dacron) aortobifemoral bypass grafts have five year patency rates of over 90% but are associated with a mortality of up to 5%. Complications include graft infection and postoperative impotence. Femoropopliteal bypass grafting, using autologous long saphenous vein, polyester, or polytetrafluoroethylene (Goretex) yields patency rates of less than 70% at five years. The early patency of prosthetic grafts seems similar to that of vein grafts, although the long term results seem less good. Femoropopliteal bypass grafts should rarely be used for patients with claudication.
Critical limb ischaemia
History and examination
Patients with critical limb ischaemia often describe a history of deteriorating claudication, progressing to nocturnal rest pain. Ulceration or gangrene commonly results from minor trauma. Nocturnal rest pain often occurs just after the patient has fallen asleep when the systemic blood pressure falls, further reducing perfusion to the foot. Hanging the foot out of bed increases perfusion and produces the typical dusky red hue due to loss of capillary tone. Elevation causes pallor and venous guttering. Inspect the foot carefully for ulceration under the heel andbetween the toes. Swelling suggests deep infection. If you can palpate foot pulses consider an alternative cause of pain, such as gout. Patients with critical limb ischaemia require urgent referral to a vascular surgeon.
Investigation
The ankle brachial systolic pressure index is usually less than 0.5. Arterial calcification may result in falsely increased pressures, and caution is needed when relying on Doppler pressures alone, especially in diabetic patients. All patients with critical limb ischaemia should ideally have arteriography with a view to endovascular treatment, if feasible. Duplex scanning may be used instead of angiography and for mapping of the long saphenous vein before distal bypass surgery. Dependent Doppler or pulse generated run off can help to determine the most suitable artery to receive a distal bypass graft if these cannot be identified by angiography.
Principles of treatment
The same principles and techniques used to treat claudication also apply to critical limb ischaemia. However, critical limb ischaemia is usually caused by multilevel disease, which means that success rates are lower. Treatment focuses on saving the limb, although modification of risk factors remains important.
Endovascular treatment
Percutaneous transluminal angioplasty or stenting of proximal disease may relieve ischaemic rest pain, but healing of ulceration or gangrene usually requires restoration of foot pulses. This may necessitate extensive angioplasty of the superficial femoral, popliteal, and tibial arteries. Good results have been reported with subintimal angioplasty. Endovascular treatment can also reduce the magnitude of subsequent surgery.
Surgery
Patients with a pattern of arterial disease considered unsuitable for endovascular treatment will usually require surgery. Fit patients with proximal disease benefit greatly from aortobifemoral bypass grafting. In unfit patients the options include crossfemoral bypass for unilateral disease or axillobifemoral bypass for bilateral disease. These extra anatomic procedures have lower patency rates. Many patients with distal disease will require bypass grafting to the popliteal or crural arteries below the knee. Autologous vein grafts give the best patency rates (70% at one year). Postoperative duplex surveillance may improve patency by permitting the detection and treatment of vein graft stenoses before occlusion occurs.
Amputation
Patients with unreconstructable peripheral vascular disease, fixed flexion deformities, or extensive tissue loss usually require a major amputation. Preservation of the knee joint has enormous advantages for wearing artificial limbs and subsequent mobility. However, there is little point in risking a non healing, below knee amputation if the patient seems unlikely to walk again. Similarly, a patient with good prospects of wearing an artificial limb will fare better with an above knee amputation, if below knee amputation seems unachievable. Local amputation of ulcerated or gangrenous toes will not heal without revascularisation.
Pain relief
Critical limb ischaemia causes severe pain that requires narcotic analgesia to provide relief. A slow release opiate such as morphine seems a good option. Opiates can be supplemented by non steroidal anti
inflammatory drugs if these are not contraindicated. Apart from rehydration, adequate analgesia alone may be the best treatment for patients with dementia or other severe comorbidity. If opiate analgesia remains inadequate, then lumbar sympathectomy (surgical or chemical) or spinal cord stimulation may help. About 20
30% of patients with critical limb ischaemia have unreconstructable disease. A meta analysis of six randomised trials of Iloprost, a stable prostacyclin analogue, found that infusion of this drug reduced the death and amputation rate. Phantom limb pain may complicate major amputation. Amitryptyline, carbamazepine, transcutaneous nerve stimulation, and acupuncture can help in this situation.
<a href="http://onlinemallstore.blogspot.com/2011/06/perfume.html/%22%3Eperfume%3C/a>
Friday, October 29, 2010
Thursday, October 28, 2010
ABC of arterial and venous disease Acute limb ischaemia
Limb ischaemia is classified on the basis of onset and severity. Complete acute ischaemia will lead to extensive tissue necrosis within six hours unless the limb is surgically revascularised. Incomplete acute ischaemia can usually be treated medically in the first instance. Patients with irreversible ischaemia require urgent amputation unless it is too extensive or the patient too ill to survive.
Clinical features
Apart from paralysis (inability to wiggle toes or fingers) and anaesthesia (loss of light touch over the dorsum of the foot or hand), the symptoms and signs of acute ischaemia are non specific or inconsistently related to its completeness. Pain on squeezing the calf indicates muscle infarction and impending irreversible ischaemia. Acute arterial occlusion is associated with intense spasm in the distal arterial tree, and initially the limb will appear “marble” white. Over the next few hours, the spasm relaxes and the skin fills with deoxygenated blood leading to mottling that is light blue or purple, has a fine reticular pattern, and blanches on pressure. At this stage the limb is still salvageable. However, as ischaemia progresses, stagnant blood coagulates leading to mottling that is darker in colour, coarser in pattern, and does not blanch. Finally, large patches of fixed staining progress to blistering and liquefaction. Attempts to revascularise such a limb are futile and will lead to life threatening reperfusion injury. In cases of real doubt the muscle can be examined at surgery through a small fasciotomy incision. It is usually obvious when the muscle is dead.
Aetiology
Acute limb ischaemia is most commonly caused by acute thrombotic occlusion of a pre existing stenotic arterial segment (60% of cases) or by embolus (30%). Distinguishing these two conditions is important because treatment and prognosis are different. Other causes are trauma, iatrogenic injury, popliteal aneurysm, and aortic dissection. More than 80% of peripheral emboli arise from the left atrial appendage in association with atrial fibrillation. They may also arise from the left ventricle, heart valves, prosthetic bypass grafts, aneurysmal disease, paradoxical embolism, and atrial myxoma (rare). In 15% of cases the source of embolus is obscure. Thrombosis in situ may arise from acute plaque rupture, hypovolaemia, or pump failure (see below).
Management
General measures
When a patient is suspected to have an acutely ischaemic limb the case must be discussed immediately with a vascular surgeon. A few hours can make the difference between death or amputation and complete recovery of limb function. If there are no contraindications (acute aortic dissection or multiple trauma, particularly serious head injury) give an intravenous bolus of heparin to limit propagation of thrombus and protect the collateral circulation.
Is angiography required?
If ischaemia is complete, the patient must be taken directly to the operating theatre because angiography will introduce delay, thrombolysis is not an option, and lack of collateral flow will prevent visualisation of the distal vasculature. If ischaemia is incomplete the patient should have preoperative angiography
since simple embolectomy or thrombectomy is unlikely to be successful, thrombolysis may be an option, and the surgeon requires a “road map” for distal bypass.
Acute embolus
Embolic occlusion of the brachial artery is not usually limb threatening, and in elderly people non
operative treatment is reasonable. Younger patients should have embolectomy to prevent subsequent claudication, especially if the dominant arm is affected. A leg affected by embolus is nearly always threatened and requires immediate surgical revascularisation. Emboli usually lodge at the common femoral bifurcation or, less commonly, the popliteal trifurcation. Femoral embolus is associated with profound ischaemia to the level of the upper thigh because the deep femoral artery is also affected. A femoral pulse does not exclude the diagnosis. Embolectomy can be done under local, regional, or general anaesthetic. The adequacy of embolectomy should be confirmed by angiography while the patient is on the operating table. On table thrombolysis should be considered if mechanical clearance has been unsuccessful. If the embolus has occurred in an area of longstanding atherosclerotic disease, surgical bypass may be necessary. Postoperatively the patient should continue to receive heparin to prevent formation of further emboli. Many surgeons postpone heparin for six hours after surgery to reduce the risk of a haematoma forming.Warfarin reduces the risk of recurrent embolism, and unless contraindicated, should be prescribed to all patients long term. Patients should not be given warfarin without first being on heparin for 48 hours since warfarin can produce a transient procoagulant state due to inhibition of the vitamin K dependent anticoagulant proteins C and S. Opinions differ about how thorough you should be in establishing the source of emboli. Transthoracic echocardiography is poor at detecting a thrombus in patients with atrial fibrillation, and a negative result does not exclude the diagnosis. Transoesophageal echocardiography provides excellent views of the left atrium but is moderately invasive and not universally available. In patients with suspected paroxysmal tachyarrhythmias, 24 hour electrocardiographic monitoring should be considered. Even if no source of embolism is found,
anticoagulation should continue long term. Although immediate loss of a limb after correctly managed acute embolus is unusual, many series report a 10 20% in hospital mortality from heart failure or recurrent embolism, particularly stroke
.
Saddle embolus
Patients with acute embolic occlusion of the aortic bifurcation have femoral pulses and appear marble white or mottled to the waist. They may also present with paraplegia due to ischaemia of the cauda equina, which can be irreversible. Immediate bilateral embolectomy restores lower limb perfusion, but many patients subsequently die from reperfusion injury.
Popliteal aneurysm
A popliteal aneurysm can initiate acute ischaemia by forming a thrombus or acting as a source of emboli. Thrombolysis is often the best treatment as simple embolectomy or thrombectomy usually leads to early rethrombosis and surgical bypass is often precluded by obliteration of the distal run off. Once the circulation is restored, a bypass should be performed to exclude the aneurysm.
Atheroembolism
Cholesterol emboli are shed from a complex, often acutely ruptured, atherosclerotic plaque. Distal pulses are usually present. The patient characteristically presents with the blue toe (finger) syndrome, which may mimic Raynaud’s phenomenon. If the blue toe syndrome is not recognised patients may deteriorate rapidly and require amputation.
Thrombosis in situ
Limbs affected by stable chronic ischaemia do not usually suddenly deteriorate without a reason—for example, silent myocardial infarction or underlying, hitherto asymptomatic, malignancy. Septicaemia, particularly pneumococcal and meningococcal, may be associated with widespread thrombosis.
Trauma
The commonest causes of non iatrogenic injury are limb fractures and dislocations (supracondylar fractures of the humerus in children, tibial fractures in adults), blunt injuries occurring in road traffic accidents, and stab wounds. In the United Kingdom, acute traumatic limb ischaemia is often iatrogenic, being caused by arterial cannulation (coronary angioplasty, aortic balloon pump), vascular and orthopaedic procedures on the limb (especially if exsanguinating tourniquets are used), or pelvic surgery (cystectomy, anterior resection) in patients with subclinical aortoiliac disease in whom the ligated pelvic collaterals form the main blood supply to the legs. Postoperative assessment of lower limb ischaemia may be confused by the presence of epidural or spinal anaesthesia. The presence of distal pulses does not exclude serious arterial injury. Pulse oximetry, Doppler signals, and measurement of the ankle brachial pressure index may be helpful, but in cases of doubt, proceed to angiography.
Intra-arterial drug administration
Intra-arterial drug administration leads to intense spasm and microvascular thrombosis. The leg is mottled and digital gangrene is common, but pedal pulses are usually palpable. The mainstay of treatment is supportive care, hydration to minimise renal failure secondary to rhabdomyolysis, and full heparinisation. Vascular reconstruction is almost never indicated, but fasciotomy may be required to prevent a compartment syndrome.
Venous gangrene
Venous gangrene can be mistaken for acute limb ischaemia. However, the leg is invariably swollen and the superficial veins full. Oedema may make it impossible to palpate pedal pulses, but Doppler examination will show normal distal waveforms and pressures. Management includes elevation, heparinisation, thrombolysis, and treatment of the underlying cause (usually pelvic or abdominal malignancy).
Aortic dissection
This may cause upper and lower limb ischaemia due to pinching of the ostia of the relevant arteries by the false lumen.
Thoracic outlet syndrome
Pressure on the subclavian artery from a cervical rib or abnormal soft tissue band may lead to a post
stenotic dilatation lined with thrombus, which predisposes to occlusion or embolisation. The distal circulation may be chronically obliterated and digital ischaemia advanced before the thoracic outlet syndrome is diagnosed. The diagnosis is based on the results of duplex ultrasonography or angiography, or both. Treatment options include thrombolysis, thrombectomy or embolectomy, excision of the cervical rib, and repair of the aneurysmal segment.
Thrombolysis
In thrombolysis a cannula is embedded into the distal extent of the thrombus and streptokinase or, preferably, recombinant tissue plasminogen activator is infused. The technique cannot be used in patients with complete ischaemia because thrombus dissolution takes several hours. It is also relatively ineffective against the organised thrombus present in most peripheral emboli and is associated with an appreciable minor (20%,
mainly groin haematoma) and major (5%, serious haemorrhage and stroke) complication rate. Thrombolysis should be undertaken only in an environment where experienced nursing and medical staff can closely monitor the patient.
Investigations of venous disease
Venous thrombosis
Colour Duplex scanning is both sensitive and specific (90 100% in most series) for detecting proximal deep vein thrombosis. Deep veins and arteries lie together in the leg, and the normal vein appears as an echo free channel and is usually larger than the accompanying artery. Venous ultrasonography is a very accurate method ofidentifying deep vein thrombi from the level of the common femoral vein at the groin crease to the popliteal vein but is less reliable for diagnosing calf vein thrombosis.
Criteria for diagnosis of deep vein thrombosis
x Failure of vein to collapse on direct compression
x Visualisation of thrombus within lumen
x Absent or abnormal venous pulsation on Doppler scanning
Venous reflux
Colour duplex scanning has revolutionised the investigation of the lower limb venous system because it allows instant visualisation of blood flow and its direction. Thus, reflux at the saphenofemoral junction, saphenopopliteal junction, and within the deep venous system, including the popliteal vein beneath the knee and the gastrocnemius veins, can be detected without invasive techniques. Although venous reflux can be assessed with a pencil Doppler, this technique misses 12% of saphenofemoral and 20% of saphenopopliteal junction reflux compared with colour duplex scanning.
Colour Duplex scanning is both sensitive and specific (90 100% in most series) for detecting proximal deep vein thrombosis. Deep veins and arteries lie together in the leg, and the normal vein appears as an echo free channel and is usually larger than the accompanying artery. Venous ultrasonography is a very accurate method ofidentifying deep vein thrombi from the level of the common femoral vein at the groin crease to the popliteal vein but is less reliable for diagnosing calf vein thrombosis.
Criteria for diagnosis of deep vein thrombosis
x Failure of vein to collapse on direct compression
x Visualisation of thrombus within lumen
x Absent or abnormal venous pulsation on Doppler scanning
Venous reflux
Colour duplex scanning has revolutionised the investigation of the lower limb venous system because it allows instant visualisation of blood flow and its direction. Thus, reflux at the saphenofemoral junction, saphenopopliteal junction, and within the deep venous system, including the popliteal vein beneath the knee and the gastrocnemius veins, can be detected without invasive techniques. Although venous reflux can be assessed with a pencil Doppler, this technique misses 12% of saphenofemoral and 20% of saphenopopliteal junction reflux compared with colour duplex scanning.
ABC OF ANTENATAL CARE
Organisation of antenatal care
Looking after pregnant women presents one of the paradoxes of modern medicine. Normal women proceeding through an uneventful pregnancy require little formal medicine. Conversely, those at high risk of damage to their own health or that of their fetus require the use of appropriate scientific technology. Accordingly, there are two classes of women, the larger group requiring support but not much intervention and the other needing the full range of diagnostic and therapeutic measures as in any other branch of medicine. To distinguish between the two is the aim of a well run antenatal service. Antenatal clinics provide a multiphasic screening service; the earlier women are screened to identify those at high risk of specified problems the sooner appropriate diagnostic tests can be used to assess such women and their fetuses and treatment can be started. As always in medicine, diagnosis must precede treatment, for unless the women who require treatment can be identified specifically, management cannot be correctly applied.
Background
Some women attend for antenatal care because it is expected of them. They have been brought up to believe that antenatal care is the best way of looking after themselves and their unborn children. This is reinforced in all educational sources from medical textbooks to women’s magazines. Prenatal care started in Edinburgh at the turn of the 20th century, but clinics for the checking of apparently well pregnant women were rare before the first world war. During the 1920s a few midwifery departments of hospitals and interested general practitioners saw women at intervals to check their urine for protein. Some palpated the abdomen, but most pregnant women had only a medical or midwifery consultation once before labour, when they booked. Otherwise, doctors were concerned with antenatal care only “if any of the complications of pregnancy should be noticed”. Obstetrics and midwifery were first aid services concerned with labour and its complications: virtually all vigilance, thought, and attention centred on delivery and its mechanical enhancement. Little attention was paid to the antenatal months. During the 1920s a wider recognition emerged of the maternal problems of pregnancy as well as those of labour; the medical profession and the then Ministry of Health woke up to realise that events of labour had their precursors in pregnancy. Janet Campbell, one of the most farsighted and clear thinking women in medicine, started a national system of antenatal
clinics with a uniform pattern of visits and procedures; her pattern of management can still be recognised today in all the clinics of the Western world. Campbell’s ideas became the clinical obstetric screening service of the 1930s. To it has been added a series of tests, often with more enthusiasm than scientific justification; over the years few investigations have been taken away, merely more added. Catalysed by the National Perinatal Epidemiological Unit in Oxford, various groups of more thoughtful obstetricians have tried to sort out which of the tests are in fact useful in predicting fetal and maternal hazards and which have a low return for effort. When this has been done a rational antenatal service may be developed, but until then we must work with a confused service that “growed like Topsy”. It is a mixture of the traditional clinical laying on of hands and a
Some women attend for antenatal care because it is expected of them. They have been brought up to believe that antenatal care is the best way of looking after themselves and their unborn children. This is reinforced in all educational sources from medical textbooks to women’s magazines. Prenatal care started in Edinburgh at the turn of the 20th century, but clinics for the checking of apparently well pregnant women were rare before the first world war. During the 1920s a few midwifery departments of hospitals and interested general practitioners saw women at intervals to check their urine for protein. Some palpated the abdomen, but most pregnant women had only a medical or midwifery consultation once before labour, when they booked. Otherwise, doctors were concerned with antenatal care only “if any of the complications of pregnancy should be noticed”. Obstetrics and midwifery were first aid services concerned with labour and its complications: virtually all vigilance, thought, and attention centred on delivery and its mechanical enhancement. Little attention was paid to the antenatal months. During the 1920s a wider recognition emerged of the maternal problems of pregnancy as well as those of labour; the medical profession and the then Ministry of Health woke up to realise that events of labour had their precursors in pregnancy. Janet Campbell, one of the most farsighted and clear thinking women in medicine, started a national system of antenatal
clinics with a uniform pattern of visits and procedures; her pattern of management can still be recognised today in all the clinics of the Western world. Campbell’s ideas became the clinical obstetric screening service of the 1930s. To it has been added a series of tests, often with more enthusiasm than scientific justification; over the years few investigations have been taken away, merely more added. Catalysed by the National Perinatal Epidemiological Unit in Oxford, various groups of more thoughtful obstetricians have tried to sort out which of the tests are in fact useful in predicting fetal and maternal hazards and which have a low return for effort. When this has been done a rational antenatal service may be developed, but until then we must work with a confused service that “growed like Topsy”. It is a mixture of the traditional clinical laying on of hands and a
patchily applied provision of complex tests, whose availability often depends as much on the whims of a health authority’s ideas of financial priority as on the needs of the women and their fetuses. As well as these economic considerations, doctors planning the care of women in pregnancy should consider the women’s own wishes. Too often antenatal clinics in the past have been designated cattle markets; the wishes of women coming for care should be sought and paid attention to. A recurrent problem is the apparent rush of the hospital clinic. The waiting time is a source of harassment and so is the time taken to travel to the clinic. Most women want time and a rapport with the antenatal doctor or midwife to ask questions and have them answered in a fashion they can understand. It is here that the midwives
come into their own for they are excellent at the care of women undergoing normal pregnancies. In many parts of the country midwives run their own clinics in places where women would go as part of daily life. Here,
midwives see a group of healthy normal women through pregnancy with one visit only to the hospital antenatal clinic.To get the best results, women at higher risk need to be screened out at or soon after booking. They will receive intensive care at the hospital consultant’s clinic and those at intermediate risk have shared care between the general practitioner and the hospital. The women at lower risk are seen by the midwives at the community clinics. Programmes of this nature now run but depend on laying down protocols for care agreed by all the obstetricians, general practitioners and midwives. Co-operation and agreement between the three groups of carers, with mutual respect and acceptance of each other’s roles, are essential. Janet Campbell started something in 1920. We should not necessarily think that the pattern she derived is fixed forever, and in the new century we may start to get it right for the current generation of women.
come into their own for they are excellent at the care of women undergoing normal pregnancies. In many parts of the country midwives run their own clinics in places where women would go as part of daily life. Here,
midwives see a group of healthy normal women through pregnancy with one visit only to the hospital antenatal clinic.To get the best results, women at higher risk need to be screened out at or soon after booking. They will receive intensive care at the hospital consultant’s clinic and those at intermediate risk have shared care between the general practitioner and the hospital. The women at lower risk are seen by the midwives at the community clinics. Programmes of this nature now run but depend on laying down protocols for care agreed by all the obstetricians, general practitioners and midwives. Co-operation and agreement between the three groups of carers, with mutual respect and acceptance of each other’s roles, are essential. Janet Campbell started something in 1920. We should not necessarily think that the pattern she derived is fixed forever, and in the new century we may start to get it right for the current generation of women.
Styles of antenatal care
The type of antenatal care that a woman and her general practitioner plan will vary with local arrangements. The important first decision on which antenatal care depends is where the baby will be delivered. Ninety seven per cent of babies in the UK are now delivered in institutions, a third of the 2.2% of domiciliary deliveries are unplanned, so about 1.5% are booked as home deliveries. If the delivery is to be in an institution there is still the choice in some areas of general practitioner deliveries either at a separate unit run by general
practitioners isolated from the hospital or in a combined unit with a consultant. Most deliveries take place in an NHS hospital under the care of a consultant team. A small but possibly increasing number in the next few years may be delivered in private care, by a general practitioner obstetrician, a consultant obstetrician, or an independent midwife. Recently a series of midwife led delivery units have been established with no residential medical cover. Once the plans for delivery are decided, the pattern of antenatal visits can be worked out. If general practitioners or midwives are going to look after delivery, antenatal care might be entirely in their hands, with the use of the local obstetric unit for investigations and consultation. At the other end of the
spectrum, antenatal care is in the hands of the hospital unit under a consultant obstetrician and a team of doctors and midwives, the general practitioner seeing little of the woman until she has been discharged from hospital after delivery. Most women, however, elect for antenatal care between these two extremes. They often wish to take a bigger part in their own care. In some antenatal clinics the dipstick test for proteinuria is done by the woman herself. As well as providing some satisfaction, this reduces the load and waiting time at the formal antenatal visit. During pregnancy there may be visits, at certain agreed stages of gestation, to the hospital antenatal clinic for crucial checks, and for the rest of the time antenatal care is performed in the general practitioner’s surgery or midwives’ clinic. These patterns of care keep the practitioner involved in the obstetric care of the woman and allow the woman to be seen in slightly more familiar surroundings and more swiftly. In some areas clinics outside the hospital are run by community midwives; these are becoming increasingly popular. Home antenatal care visits also take place, including the initial booking visit. Delivery may be in the hospital by the consultant led team, by a general practitioner obstetrician, or by a midwife. It is wise, with the introduction of Crown indemnity, that all general practitioner obstetricians have honorary contracts with the hospital obstetric department that they attend to supervise or perform deliveries. About 2% of women now have a home delivery. More than half of these are planned and for this group, antenatal care may well be midwifery led (see ABC of Labour Care).
spectrum, antenatal care is in the hands of the hospital unit under a consultant obstetrician and a team of doctors and midwives, the general practitioner seeing little of the woman until she has been discharged from hospital after delivery. Most women, however, elect for antenatal care between these two extremes. They often wish to take a bigger part in their own care. In some antenatal clinics the dipstick test for proteinuria is done by the woman herself. As well as providing some satisfaction, this reduces the load and waiting time at the formal antenatal visit. During pregnancy there may be visits, at certain agreed stages of gestation, to the hospital antenatal clinic for crucial checks, and for the rest of the time antenatal care is performed in the general practitioner’s surgery or midwives’ clinic. These patterns of care keep the practitioner involved in the obstetric care of the woman and allow the woman to be seen in slightly more familiar surroundings and more swiftly. In some areas clinics outside the hospital are run by community midwives; these are becoming increasingly popular. Home antenatal care visits also take place, including the initial booking visit. Delivery may be in the hospital by the consultant led team, by a general practitioner obstetrician, or by a midwife. It is wise, with the introduction of Crown indemnity, that all general practitioner obstetricians have honorary contracts with the hospital obstetric department that they attend to supervise or perform deliveries. About 2% of women now have a home delivery. More than half of these are planned and for this group, antenatal care may well be midwifery led (see ABC of Labour Care).
Early diagnosis of pregnancy
When a woman attends a practitioner thinking that she is pregnant, the most common symptoms are not always amenorrhoea followed by nausea. Many women, particularly the multiparous, have a subtle sensation that they are pregnant a lot earlier than the arrival of the more formal symptoms and signs laid down in textbooks. Traditionally, the doctor may elicit clinical features, but most now turn to a pregnancy test at the first hint of pregnancy. Symptoms The symptoms of early pregnancy are nausea, increased sensitivity of the breasts and nipples, increased frequency of micturition, and amenorrhoea.
Signs
The doctor may notice on examination a fullness of the breasts with early changes in pigmentation and Montgomery’s tubercuiles in the areola. The uterus will not be felt through the abdominal wall until about 12 weeks of pregnancy. On bimanual assessment uterine enlargement is detectable before this time while cervical softening and a cystic, generally soft feeling of the uterus can be detected by eight weeks. This more subtle sign is not often sought as vaginal examination is not usually performed on a normal woman at this time.
Tests
Mostly the diagnosis of pregnancy is confirmed by tests checking for the higher concentrations of human chorionic gonadotrophin that occur in every pregnancy. The old biological tests using rabbits and frogs are now gone and have been replaced by immunological tests. These depend on the presence of human chorionic gonadotrophin in the body fluids, which is reflected in the urine. The more sensitive the test, the more likely it is to pick up the hormone at lower concentrations—that is, earlier in pregnancy. Enzyme linked immunosorbent assay (ELISA) is the basis of many of the commercial kits currently available in chemist
shops. The assay depends on the double reaction of standard phase antibody with enzyme labelled antibody, which is sensitive enough to detect very low concentrations of human chorionic gonadotrophin. Positive results may be therefore detectable as early as 10 days after fertilisation—that is, four days before the first missed period. Vaginal ultrasound can detect a sac from five weeks and a fetal cardiac echo a week or so later (Chapter 4), but this would not be used as a screening pregnancy test.
Conclusion
At the end of the preliminary consultation women may ask questions about the pregnancy and the practitioner will deal with these. Most of these queries will be considered in the chapter on normal antenatal management. For most women the onset of pregnancy is a desired and happy event, but for a few it may not be so and practitioners, having established a diagnosis, may find that they are then asked to advise on termination of pregnancy. This they should do if their views on the subject allow; if not, they should arrange for one of their partners to discuss it with the patient. Most women, however, will be happy to be pregnant and looking forward to a successful outcome.
Investigations of arterial disease
Ankle brachial pressure index
Under normal conditions, systolic blood pressure in the legs is equal to or slightly greater than the systolic pressure in the upper limbs. In the presence of an arterial stenosis, a reduction in pressure occurs distal to the lesion. The ankle brachial pressure index, which is calculated from the ratio of ankle to brachial systolic pressure, is a sensitive marker of arterial insufficiency. The highest pressure measured in any ankle artery is used as the numerator in the calculation of the index; a value >1.0 is normal and a value < 0.9 is abnormal. Patients with claudication tend to have ankle brachial pressure indexes in the range 0.5 0.9, whereas those with critical ischaemia usually have an index of < 0.5. The index also has prognostic significance because of the association with arterial disease elsewhere, especially coronary heart disease.
Diabetic limbs
Systolic blood pressure in the lower limbs cannot be measured reliably when the vessels are calcified and incompressible—for example, in patients with diabetes—as this can result in falsely high ankle pressures. An alternative approach is to use either the pole test or measurement of toe pressures. Normal toe systolic pressure ranges from 90 100 mm Hg and is 80 90% of brachial systolic pressure. A toe systolic pressure < 30 mm Hg indicates critical ischaemia.
Walk test
Exercise testing will assess the functional limitations of arterial stenoses and differentiate occlusive arterial disease from other causes of exercise induced lower limb symptoms—for example, neurogenic claudication secondary to spinal stenosis. A limited inflow of blood in a limb with occlusive arterial disease results
in a fall in ankle systolic blood pressure during exercise induced peripheral vasodilatation. The walk test is performed by exercising the patient for 5 minutes, ideally on a treadmill, but walking the patient in the
surgery or marking time on the spot are adequate. The ankle brachial pressure index is measured before and after exercise. A pressure drop of 20% or more indicates significant arterial disease. If there is no drop in ankle systolic pressure after a 5 minute brisk walk, the patient does not have occlusive arterial disease proximal to the ankle in that limb.
Duplex scanning
Duplex ultrasonography has a sensitivity of 80% and a specificity of 90 100% for detecting femoral and popliteal disease compared with angiography, but it is less reliable for assessing the severity of stenoses in the tibial and peroneal arteries. Duplex scanning is especially useful for assessing the carotid arteries and for surveillance of infrainguinal bypass grafts where sites of stenosis can be identified before complete graft occlusion occurs and before there is a fall in ankle brachial pressure index. The normal velocity within a graft conduit is 50 120 cm/s. As with native arteries, a twofold increase in peak systolic velocity indicates a stenosis of 50% or more. A peak velocity < 45 cm/s occurs in grafts at high risk of failure.
Identification of distal vessels for arterial bypass grafting
In critically ischaemic limbs, where occlusive disease tends to be present at multiple levels, arteriography often fails to show patent calf or pedal vessels as potential outflows for femorodistal bypass grafting. Alternative non invasive approaches have been developed for preoperative assessment, including pulse generated run off and dependent Doppler assessment.
Transcranial Doppler ultrasonography
Lower frequency Doppler probes (1 2 MHz) can be used to obtain information about blood flow in arteries comprising the circle of Willis and its principal branches. Mean flow velocities > 80 cm/s in the middle cerebral artery, or > 70 cm/s in the posterior and basilar arteries, indicate a serious stenosis. Transcranial Doppler scanning has several applications but is especially useful for intraoperative and postoperative monitoring of patients having carotid endarterectomy.
Helical or spiral computed tomography
Spiral computed tomography is a new, minimally invasive technique for vascular imaging that is made possible by combining two recent advances: slip ring computed tomography (which allows the x ray tube detector apparatus to rotate continuously) and computerised three dimensional reconstruction. A helical scan can cover the entire region of interest (for example, the abdominal aorta from the diaphragm to the iliac bifurcation) in one 30 40 second exposure, usually in a single breath hold. This minimises motion artefact and allows all the scan data to be collected during the first pass of an intravenous bolus of contrast through the arterial tree—that is during the time of maximal arterial opacification. A large number of finely spaced slices from one scan can then be reconstructed to produce high quality two or three dimensional images of the contrast enhanced vessels.
Magnetic resonance angiography
Magnetic resonance angiography has developed rapidly over the past five years. It has the advantage of imaging a moving column of blood and does not require ionising radiation or iodinated contrast, but the technique has obvious drawbacks in terms of cost efficiency and accessibility to scanners. A variety of
imaging sequences are used depending on the vessels being studied and the field strength of the machine. The most commonly used techniques include time of flight, two and three dimensional angiography and phase contrast. Use of a magnetic resonance imaging scanner with a high field strength (which allows rapid acquisition of data) and a carefully timed bolus of gadolinium contrast enables high quality angiographic images to be obtained in a single breath hold. Magnetic resonance angiography is well established for examining the cerebral vessels and the car
ABC of arterial and venous disease
Noninvasive methods of arterial and venous assessment
Although diagnostic and therapeutic decisions in patients with vascular disease are guided primarily by the history and physical examination, the use of non invasive investigations has increased significantly in recent years, mainly as a result of technological advances in ultrasonography. This article describes the main investigative techniques.
Principles of vascular ultrasonography
In the simplest form of ultrasonography, ultrasound is transmitted as a continuous beam from a probe that contains two piezoelectric crystals. The transmitting crystal produces ultrasound at a fixed frequency (set by the operator according to the depth of the vessel being examined), and the receiving crystal vibrates in response to reflected waves and produces an output voltage. Conventional B mode (brightness mode) ultrasonography records the ultrasound waves reflected from tissue interfaces, and a two dimensional picture is built up according to the reflective properties of the tissues.
Doppler ultrasonography
Ultrasound signals reflected off stationary surfaces retain thesame frequency with which they were transmitted, but the principle underlying Doppler ultrasonography is that the frequency of signals reflected from moving objects such as red blood cells shifts in proportion to the velocity of the target. The output from a continuous wave Doppler ultrasonograph is usually presented as an audible signal, so that a sound is heard whenever there is movement of blood in the vessel being examined.
Pulsed ultrasonography
Continuous wave ultrasonography provides little scope for restricting the area of tissue that is being examined because any sound waves that are intercepted by the receiving crystal will produce an output signal. The solution is to use pulsed ultrasonography. The investigator can focus on a specific tissue plane by transmitting a pulse of ultrasound and closing the receiver except when signals from a predetermined depth are returning. This allows, for example, the centre of an artery and the areas close to the vessel wall to be examined in turn.
Duplex scanners
An important advance in vascular ultrasonography has been the development of spectral analysis, which delineates the complete spectrum of frequencies (that is, blood flow velocities) found in the arterial waveform during a single cardiac cycle. The normal (“triphasic”) Doppler velocity waveform is made up of three components which correspond to different phases of arterial flow: rapid antegrade flow reaching a peak during systole, transient reversal of flow during early diastole, and slow antegrade flow during late diastole. Doppler examination of an artery distal to a stenosis will show characteristic changes in the velocity profile: the rate of rise is delayed, the amplitude decreased, and the transient flow reversal in early diastole is lost. In severe disease, the Doppler waveform flattens; in critical limb ischaemia it may be undetectable. Examination of an arterial stenosis shows an increase in blood velocity through the area of narrowing. The site(s) of any stenotic lesions can be identified by serial placement of the Doppler probe along the extremities. The criteria used to define a stenosis vary between laboratories, but a twofold increase in peak systolic velocity compared with the velocity in an adjacent segment
By combining the pulsed Doppler system with real time B mode ultrasound imaging of vessels, it is possible to examine Doppler flow patterns in a precisely defined area within the vessel lumen. This combination of real time B mode sound imaging with pulsed Doppler ultrasonography is called duplex scanning. The addition of colour frequency mapping (so called colour duplex or triplex scanners) makes the identification of arterial stenoses even easier and reduces the scanning tim
Friday, October 8, 2010
Anatomy of Olfactory System
Introduction The olfactory system represents one of the oldest sensory modalities in the phylogenetic history of mammals. Olfaction is less developed in humans than in other mammals such as rodents. As a chemical sensor, the olfactory system detects food and influences social and sexual behavior. The specialized olfactory epithelial cells characterize the only group of neurons capable of regeneration. Activation occurs when odiferous molecules come in contact with specialized processes known as the olfactory vesicles. Within the nasal cavity, the turbinates or nasal conchae serve to direct the inspired air toward the olfactory epithelium in the upper posterior region. This area (only a few centimeters wide) contains more than 100 million olfactory receptor cells. These specialized epithelial cells give rise to the olfactory vesicles containing kinocilia, which serve as sites of stimulus transduction.
The image below depicts olfactory anatomy.
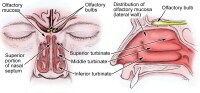 Head anatomy with olfactory nerve.
Head anatomy with olfactory nerve.Olfactory Epithelium
The olfactory epithelium consists of 3 cell types, basal, supporting, and olfactory receptor cells. Basal cells are stem cells that give rise to the olfactory receptor cells. The continuous turnover and new supply of these neurons are unique to the olfactory system. In no other location in the mature nervous system do less differentiated stem cells replace neurons. Supporting cells are scattered among the receptor cells and have numerous microvilli and secretory granules, which empty their contents onto the mucosal surface. The receptor cells are actually bipolar neurons, each possessing a thin dendritic rod that contains specialized cilia extending from the olfactory vesicle and a long central process that forms the fila olfactoria. The cilia provide the transduction surface for odorous stimuli.
The vomeronasal organ is a specialized bilateral membranous structure located in the base of the anterior nasal septum, at the junction of the septal cartilage and the bony septum. It is believed to detect external chemical signals called pheromones. These signals, which are not detected consciously as odors by the olfactory system, mediate human autonomic, psychological, and endocrine responses.
The trigeminal nerve innervates the posterior nasal cavity to detect noxious stimuli.
Olfactory Nerve and the Cribriform Plate
The small unmyelinated axons of the olfactory receptor cells form the fine fibers of the first cranial nerve and travel centrally toward the ipsilateral olfactory bulb to make contact with the second-order neurons. Conduction velocities are extremely slow, and support is provided in bundles by a single Schwann cell. As previously mentioned, the trigeminal nerve (cranial nerve V) sends fibers to the olfactory epithelium to detect caustic chemicals such as ammonia. The cribriform plate of the ethmoid bone, separated at the midline by the crista galli, contains multiple small foramina through which the olfactory nerve fibers, or fila olfactoria, traverse. Fracture of the cribriform plate in traumatic settings can disrupt these fine fibers and lead to olfactory dysfunction.
Olfactory Bulb
The olfactory bulb lies inferior to the basal frontal lobe. The olfactory bulb is a highly organized structure composed of several distinct layers and synaptic specializations. The layers (from outside toward the center of the bulb) are differentiated as follows:
- Glomerular layer
- External plexiform layer
- Mitral cell layer
- Internal plexiform layer
- Granule cell layer
Mitral cells are second-order neurons contacted by the olfactory nerve fibers at the glomerular layer of the bulb. The glomerular layer is the most superficial layer, consisting of mitral cell dendritic arborizations (glomeruli), olfactory nerve fibers, and periglomerular cells. Periglomerular cells contact multiple mitral cell dendrites within the glomeruli and provide lateral inhibition of neighboring glomeruli while allowing excitation of a specific mitral cell dendritic tree. Each mitral cell is contacted by at least 1000 olfactory nerve fibers.
The external plexiform layer contains the passing dendrites of mitral cells and a few tufted cells, which are similar in size to mitral cells. Some of the granule cell dendrites in the plexiform layer contact mitral cell dendrites through a specialized dendrodendritic synapse, which also is termed a reciprocal synapse (vesicles seen within both presynaptic and postsynaptic membranes).
Tufted cells also receive granule cell input through dendrodendritic and dendrosomatic contact. Pyramidal mitral cells are the largest neurons in the bulb and are located in a narrow band between the external and internal plexiform layers. The granule cell layer contains multiple small round neurons that lack axons. Long dendritic processes of the neurons reach the more superficial layers and inhibit mitral cells and tufted cells. Small distal processes make contacts with the exiting mitral cell axons.
Olfactory Tract and Central Pathways
Mitral cell axons project to the olfactory cortex via the olfactory tract. Medial fibers of the tract contact the anterior olfactory nucleus and the septal area. Some fibers project to the contralateral olfactory bulb via the anterior commissure. Lateral fibers contact third-order neurons in the primary olfactory cortex (prepyriform and entorhinal areas) directly. Third-order neurons send projections to the dorsomedial nucleus of the thalamus, the basal forebrain, and the limbic system.
The thalamic connections are thought to serve as a conscious mechanism for odor perception, while the amygdala and the entorhinal area are limbic system components and may be involved in the affective components of olfaction. Investigations of regional cerebral blood flow have demonstrated a significant increase in the amygdaloid nucleus with the introduction of a highly aversive odorant stimulus, and this has been associated with subjective perceived aversiveness.
Central Projections
The pyriform lobe includes the olfactory tract, the uncus, and the anterior part of the parahippocampal gyrus. The prepyriform and the periamygdaloid areas of the temporal lobe represent the primary olfactory cortex. The entorhinal area is known as the secondary olfactory cortex and is included in the pyriform lobe. The olfactory system is the only sensory system that has direct cortical projections without a thalamic relay nucleus. The dorsomedial nucleus of the thalamus receives some olfactory fibers that ultimately reach the orbitofrontal cortex.
The anterior olfactory nucleus receives collateral fibers from the olfactory tract and projects to the contralateral olfactory bulb and anterior olfactory nucleus via the anterior commissure.
The region of anterior perforated substance contains cells that receive direct mitral cell collaterals and input from the anterior olfactory nucleus, amygdaloid nucleus, and temporal cortex. This area ultimately projects to the stria medullaris and the medial forebrain bundle.
Using the uncinate fasciculus, the entorhinal area sends projections to the hippocampal formation, anterior insula, and frontal cortex.
Clinical Correlation
As many as 2 million people in the United States experience some type of olfactory dysfunction, causes of which include head trauma, upper respiratory infections, tumors of the anterior cranial fossa, and exposure to toxic chemicals or infections. The following terms are used to describe the degree of smell aberration:
- Anosmia - Absence of smell sensation
- Hyposmia - Decreased sensation
- Dysosmia - Distortion of smell sensation
- Cacosmia - Sensation of a bad or foul smell
- Parosmia - Sensation of smell in the absence of appropriate stimulus
Olfactory dysfunction is a hallmark of certain syndromes such as Kallmann syndrome (ie, hypogonadism with anosmia) and Foster Kennedy syndrome (ie, papilledema, unilateral anosmia, and optic atrophy usually associated with an olfactory groove meningioma).
The classic description of partial complex epilepsy with a mesial temporal focus includes an aura of foul-smelling odors (termed uncinate fits) that occur before seizure onset, emphasizing presumed origination at the uncus.
Olfactory dysfunction is associated with early Parkinson disease and with other neurodegenerative disorders such as Alzheimer disease and Huntington chorea.1 An association also exists between abnormal olfactory identification and obsessive-compulsive disorder.2
Head trauma leading to fracture of the cribriform plate may cause cerebrospinal fluid (CSF) rhinorrhea and a potential for meningitis. Paranasal sinus endoscopy may lead to violation of the cribriform plate and potential infectious complications. Olfactory structures also can be injured during craniotomies involving the anterior cranial base or from subarachnoid hemorrhage, which may disrupt the fine fibers of the olfactory nerve.
Clinical Evaluation
Detection of olfactory dysfunction begins with sampling of a series of common odors, which can be performed at the bedside with odiferous substances such as coffee, lemon, and peppermint. Tests, including those developed at the Connecticut Chemosensory Clinical Research Center (CCCRC), have aided examiners in identification of abnormalities in odor detection and discrimination. The University of Pennsylvania Smell Identification Test (UPSIT) is another useful tool; it consists of 40 items for evaluation of olfactory and trigeminal nerve function in the nasal cavity.
Central hyposmia may manifest as abnormalities in odor recognition rather than odor detection. Thorough evaluation of patients who have anosmia includes imaging of anterior cranial structures. The clinician should always counsel patients with anosmia regarding sensory loss, including potential risks associated with the lack of smell sensation (eg, inability to detect dangers such as smoke, spoiled foods, toxins).
Promptly complete evaluation and treatment of clear rhinorrhea in the patient in whom leakage of CSF is suspected. Initial testing of fluid for glucose suggests CSF but is not confirmatory. Presence of beta-transferrin is a more sensitive indicator of CSF rhinorrhea. Computed tomography with cisternography or radionuclide scans can be used to detect the site of CSF leakage from the anterior cranial fossa. Repair of leaks at the level of the cribriform plate may be achieved from the intracranial approach, intranasal (endoscopic) approach, or both, depending on the nature of the defect.
Positron emission tomography (PET) and functional MRI are promising modalities to assist in making the diagnosis of different types of hyposmia (central vs peripheral), as well as in delineation of the role of limbic structures as sites of odor recognition, memory, and integration of multisensory inputs.
Subscribe to:
Posts (Atom)